Conditions – Colon and Rectum
Colorectal polyps
Being told you have a polyp, or reading about them after noticing a symptom, often prompts the same concern: does this mean cancer? In the majority of cases, it does not. The full picture is more layered than that, however, and understanding the detail tends to ease a great deal of worry.
Dr Georgios Markides CCT (UK), a Consultant General and Colorectal Surgeon based in Nicosia, diagnoses and removes these growths as a routine part of his practice. This guide explains what colorectal polyps are, the various types, why they develop, and when they require attention. The aim is clarity, written for patients rather than clinicians.
What Exactly Is a Polyp?
A clear definition is the right place to begin.
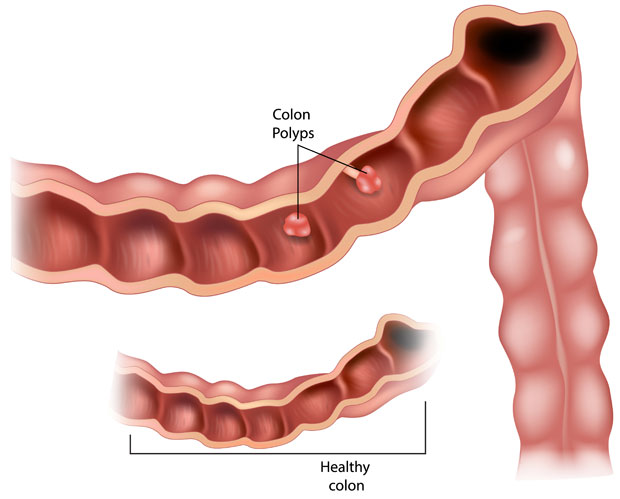
Colorectal polyps are small growths that develop on the lining of the large intestine or the rectum. They appear as raised areas rising from the inner surface of the bowel wall. Some remain flat and barely perceptible. Others form on a stalk, resembling a small mushroom. In essence, they are mucosal growths that protrude into the channel through which waste passes.
These lesions are also referred to as colonic polyps, or bowel polyps, in everyday language. Regardless of the term used, the underlying concept is consistent: an abnormal growth of tissue where none should be. Most measure only a few millimetres, while a smaller number enlarge gradually over a period of years.
There is an important reassurance here. Most colon polyps are harmless and will never produce any difficulty. The reason clinicians monitor them closely is that a minority can change over time, and identifying which ones matters.
The Different Types of Polyps
Polyps are not a single entity, and the type carries considerable significance. Clinicians divide them into two broad groups according to their behaviour.
Neoplastic Versus Non-Neoplastic
The first category, non-neoplastic polyps, rarely becomes dangerous and typically causes no harm. The second, neoplastic polyps, carries a genuine potential to turn cancerous if left untreated over a sufficient period. This distinction informs nearly every clinical decision that follows a diagnosis.
A Closer Look at Each Kind
The principal varieties include:
- Adenomatous polyps, also known as adenomas. These represent the most common precancerous type, which is why removal is generally recommended.
- Hyperplastic polyps, frequently encountered and almost always benign, particularly in the lower bowel.
- Serrated polyps, a more complex group; certain sessile forms follow their own pathway towards malignancy, while others remain harmless.
- Hamartomatous polyps, often associated with inherited conditions, composed of normal tissue arranged in a disorganised pattern.
- Juvenile polyps, usually seen in children, commonly single and benign, though multiple growths warrant assessment.
|
Polyp Type |
Category |
Cancer Risk |
|
Hyperplastic |
Non-neoplastic |
Very low |
|
Inflammatory |
Non-neoplastic |
Low, indicates inflammation |
|
Hamartomatous |
Mostly non-neoplastic |
Low, higher if numerous |
|
Adenomatous (tubular, villous) |
Neoplastic |
Moderate to high with size |
|
Serrated (sessile) |
Neoplastic pathway |
Variable, can be significant |
Setting the types out side by side clarifies an important point. A small hyperplastic growth differs markedly from a large villous adenoma, even though both share the same general name.
Symptoms You Might Notice
A frequent challenge in clinical practice concerns how quietly these growths behave.
The majority produce no symptoms whatsoever. Many people carry a polyp for years without any awareness of it, and learn of its presence only during an unrelated examination. That silence is precisely what makes regular screening so valuable.
When larger growths do cause noticeable effects, the warning signs may include:
- Blood in the stool, which can appear bright red or considerably darker.
- A small quantity of mucus passed during a bowel movement.
- A persistent change in normal bowel habits, whether looser motions or constipation.
- Abdominal cramps or discomfort that does not resolve.
- Fatigue linked to a low iron level, resulting from slow, unnoticed bleeding.
None of these features confirms a polyp, and certainly not cancer. Haemorrhoids cause bleeding as well, and many benign conditions disturb digestion. Even so, if blood or a lasting change continues for three weeks or longer, medical assessment is advisable. A precautionary appointment is always preferable to a delayed diagnosis.
Why Do Polyps Form?
Establishing a precise cause is difficult because no single trigger has been identified.
The bowel lining renews itself continuously, shedding older cells and generating new ones in a generally orderly sequence. On occasion, that process falters. The body produces a surplus of cells, they accumulate, and a small mass forms. These slow-growing overgrowths develop gradually, frequently across a decade or more, which explains the strong association with age.
Heredity also contributes. Some individuals inherit a predisposition to form them, and in rarer instances, specific genetic faults are responsible. Those inherited conditions are addressed later, as they substantially alter the management approach.
Who Is More Likely to Get Them?
Several factors raise the likelihood. Some can be modified, while others lie beyond personal control.
Influences that increase the chance of developing polyps include:
- Age over 50: Roughly one in four people beyond this point has at least one growth.
- Family history: A close relative affected by polyps or bowel cancer elevates individual risk.
- Inflammatory bowel diseases such as ulcerative colitis or Crohn’s, both of which inflame the gut over extended periods.
- Smoking and heavy alcohol consumption, a pairing that appears to worsen the outlook.
- Excess weight and physical inactivity, alongside a diet rich in red or processed meat.
Age and family history cannot be altered. Lifestyle, by contrast, remains within reach: stopping smoking, increasing activity, improving diet, and maintaining a healthy weight all reduce risk in a measurable way.
The Link Between Polyps and Cancer
This connection is the central concern for most patients, and it merits a careful explanation.
A point worth stating plainly: having a polyp does not mean cancer is present, nor that it will inevitably develop. The overwhelming majority never progress. At the same time, most cases of colorectal cancer do originate in a polyp that remained in place for many years, changing slowly. Both statements hold true simultaneously.
Where progression does occur, it tends to be gradual. An adenoma might require a decade to become malignant, sometimes considerably longer. That extended interval represents a genuine clinical advantage. It allows ample opportunity to detect and remove the growth before anything harmful arises. Removing a polyp early therefore prevents a cancer that could otherwise have formed.
Larger growths and particular types present greater concern than others. A 2 millimetre hyperplastic spot does not warrant the same caution as a centimetre-wide villous adenoma. Size, type, and number each influence the level of clinical vigilance applied.
How Polyps Are Found
Because symptoms are so often absent, detection generally depends on examining the bowel directly. Two principal methods are available.
Colonoscopy
A colonoscopy remains the reference standard. A slender, flexible instrument fitted with a camera passes gently through the colon, allowing the surgeon to inspect the full length of the lining in real time. Its key strength lies in both diagnosis and treatment: a polyp identified during the examination can frequently be removed in the same session. Dr Markides is an accredited colonoscopist certified by the Joint Advisory Group (JAG) in the UK, and can refer you to the appropriate specialist.
CT Colonography
For certain patients, a CT colonography provides an alternative. The scan combines X-rays and computer imaging to produce a detailed view of the bowel and highlight any growths without an instrument being introduced. It cannot remove anything, so a positive finding is typically followed by a colonoscopy.
After a polyp has been excised, it is sent to a laboratory. Specialists then confirm whether it was fully removed, establish its type, and check for any concerning changes. That report determines what further steps, if any, are required.
Treatment and Removal
Once a polyp has been identified, removal is the usual recommendation, and the process is frequently far simpler than patients anticipate.
Polypectomy
The most common technique, polypectomy, takes place during a colonoscopy. A fine wire loop encircles the growth and either snips or cauterises it away. No incisions are involved, no overnight admission is needed, and the procedure causes no real discomfort. Small growths are dealt with in seconds.
Endoscopic Mucosal Resection
For flatter or larger lesions, endoscopic mucosal resection (EMR) raises the growth from the bowel wall before excising it, again entirely through the scope. This requires refined technical skill, which Dr Markides applies as part of his colorectal practice.
When Surgery Is Needed
In a minority of cases, where polyps are very large, very numerous, or awkwardly positioned, keyhole surgery offers the safer route to remove a section of the bowel. Such situations are the exception. When an operation is required, Dr Markides completes these procedures laparoscopically in over 95 per cent of cases, which generally means less pain and a faster recovery. Dr Markides also performs Transanal Minimally Invasive Surgery (TAMIS) for selected large rectal growths, a service he established during his hospital career in the United Kingdom.
|
Situation |
Usual Approach |
Setting |
|
Small polyp found at colonoscopy |
Polypectomy (snare or cauterise) |
Same procedure |
|
Flat or larger lesion |
Endoscopic mucosal resection |
Same or follow-up procedure |
|
Very large or numerous growths |
Keyhole or transanal surgery |
Planned operation |
Inherited Polyp Conditions
A small proportion of people inherit genetic changes that cause polyps to form in large numbers. These conditions deserve separate consideration, because the management principles differ.
Several polyposis syndromes belong to this category. Familial adenomatous polyposis (FAP) produces hundreds or thousands of growths from an early age, and the cancer risk without treatment is exceptionally high. Lynch syndrome may, by contrast, generate relatively few polyps, yet those can become cancerous rapidly. Juvenile polyposis syndrome and Peutz-Jeghers syndrome are rarer still, though both raise long-term risk.
Individuals affected by any of these conditions require closer surveillance, frequently beginning screening much earlier than the general population and repeating it more often. Genetic counselling forms part of that approach. Where bowel cancer features prominently in a family, particularly at younger ages, raising the matter with a specialist is sensible, since it reshapes the entire monitoring plan.
Your Care with Dr Markides in Cyprus
The clinician performing the procedure matters, because polyp management combines technical precision with sound judgement, and experience is evident in both.
Dr Georgios Markides trained for seventeen years across the United Kingdom, graduating with honours from the University of Manchester before completing higher surgical training in major teaching hospitals. He holds the Certificate of Completion of Training (CCT) from the General Medical Council, a Master’s degree in Advanced Surgical Practice awarded with Distinction, and recognition from the Association of Coloproctology of Great Britain and Ireland for his colorectal subspecialty. In 2016, he became a permanent Consultant Colorectal Surgeon at the Royal Blackburn Teaching Hospital, managing thousands of emergency and elective cases. After moving his practice to Cyprus in 2018, he has performed thousands more procedures. His focus lies in advanced colorectal cancer surgery, personally undertaking over 100 major colorectal oncological operations each year, with a laparoscopic success rate above 95 per cent. As a JAG-accredited colonoscopist, he has also carried out thousands of diagnostic examinations.
Patients frequently comment on his manner as much as his credentials. He explains each step without haste, addresses difficult questions directly, and treats those in his care as individuals. Based at the Apex Building in Strovolos, Nicosia, the clinic serves patients from across Cyprus, including Larnaca, Limassol, Paphos and Famagusta, with on-site diagnostics that keep the process efficient.
Frequently Asked Questions
Are all colorectal polyps cancerous?
No, and this remains a common misconception worth correcting. The large majority of polyps are benign and never develop into cancer, particularly hyperplastic and small inflammatory types. Only certain neoplastic polyps, principally adenomas and some serrated lesions, carry a genuine chance of becoming malignant, and even then the change usually unfolds over many years. Removal during a colonoscopy effectively interrupts that process. Dr Georgios Markides assesses each growth individually and arranges laboratory analysis to confirm its precise nature.
How quickly can a polyp turn into cancer?
Progression, where it happens at all, is generally slow. An adenomatous polyp may take approximately ten years to become cancerous, although some advance more quickly and many never do. Size and type affect the pace, with larger growths carrying greater risk. This lengthy timeframe is the reason regular screening proves so effective, since it identifies polyps well before any harmful transformation. Patients with inherited polyposis conditions can progress faster and require closer monitoring under specialist supervision.
Is removing a polyp painful?
For most people, it is not. A standard polypectomy during colonoscopy is painless, because the bowel lining lacks the pain receptors found in skin. The examination itself may feel mildly uncomfortable owing to air and movement, yet the removal is not felt. Sedation is usually offered to keep you relaxed throughout. Larger growths requiring endoscopic mucosal resection or surgery involve a longer recovery, which Dr Markides discusses fully beforehand so the process is clear in advance.
How often should I have a colonoscopy after polyps are found?
The interval depends on the findings. Patients with one or two small low-risk growths may wait five to ten years before the next examination, whereas those with larger, multiple, or higher-risk adenomas might need repeat surveillance within three years. Family history and inherited conditions shorten that gap further. Your surgeon sets a personalised schedule based on the laboratory results and overall risk profile, rather than applying a single fixed rule to every individual.
Can diet and lifestyle prevent bowel polyps?
To an extent, yes, though no measure eliminates the risk entirely. A diet rich in fibre from fruit, vegetables and whole grains, reducing red and processed meat, limited alcohol, regular activity, and stopping smoking all lower the likelihood of developing polyps. Maintaining a healthy weight also helps. These steps complement screening rather than replacing it, since some growths form regardless of lifestyle, particularly where genetics or inflammatory conditions play a part.
Concerned About Your Bowel Health? Find Out More
There is no need to remain uncertain. Whether a symptom has caused concern, or your family history weighs on your mind, clear answers are readily available. Dr Georgios Markides offers honest guidance, UK-trained expertise, and a considered, attentive approach here in Cyprus.
Read more about screening and diagnosis, or learn how Dr Markides supports patients through each stage of their care.
Choose Category
– Colorectal cancer
– Colorectal polyps
– Diverticulosis
– Ulcerative colitis and Crohn’s
– Stoma
– Abdominal pain
– Constipation
Need to contact us or book an appointment?
Disclaimer
The information relating to general and colorectal disorders and their treatments given on this website is not complete and is not intended as a substitute for a consultation with your doctor. Always seek medical advice from your doctor before making a decision about any of the conditions and/or treatments mentioned on this website.
© Dr Georgios Markides
Contact Information
You can always contact our Clinic for booking appointments and other useful information:
Dr. Georgios Markides,
Consultant General & Colorectal Surgeon
APEX Building, 47 Andreas Avraamides Str., 2024 Strovolos, Nicosia, Cyprus
+357-22-282008