Conditions – Colon and Rectum
Colorectal cancer
A diagnosis involving the bowel, or even the worry of one, can feel frightening and a little isolating too. Most people arrive with a head full of questions they were too anxious to ask anyone else. That is normal. Dr Georgios Markides CCT (UK), a Consultant General and Colorectal Surgeon based in Nicosia, has spent his career sitting on the other side of those conversations, and his view is simple: the more you understand, the less power the fear holds over you.
This guide explains what colorectal cancer is, the warning signs worth taking seriously, how it’s detected, and a plain overview of how it’s managed. No jargon for the sake of it. Just the things patients tend to want explained properly, before they decide what to do next.
What Colorectal Cancer Really Is
Let’s start with the basics, because the name itself confuses people.
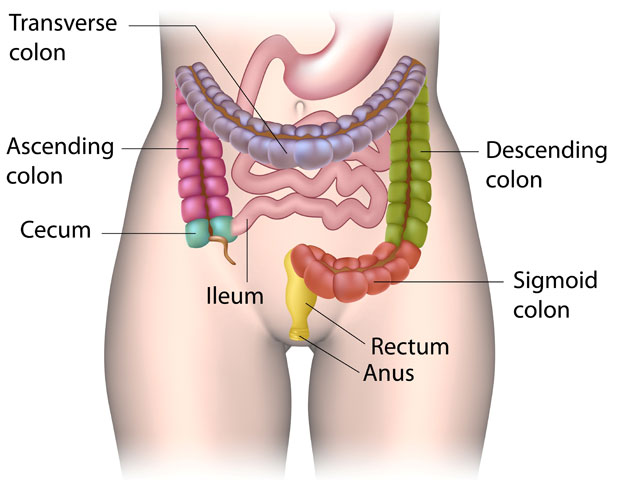
Colorectal cancer is a disease that develops in the lower digestive system, specifically the colon or the rectum. The colon makes up most of the large intestine, while the rectum is the final stretch before waste leaves the body. When doctors lump the two together, they call it colorectal because tumours in both areas behave in broadly similar ways and are usually handled by the same specialist.
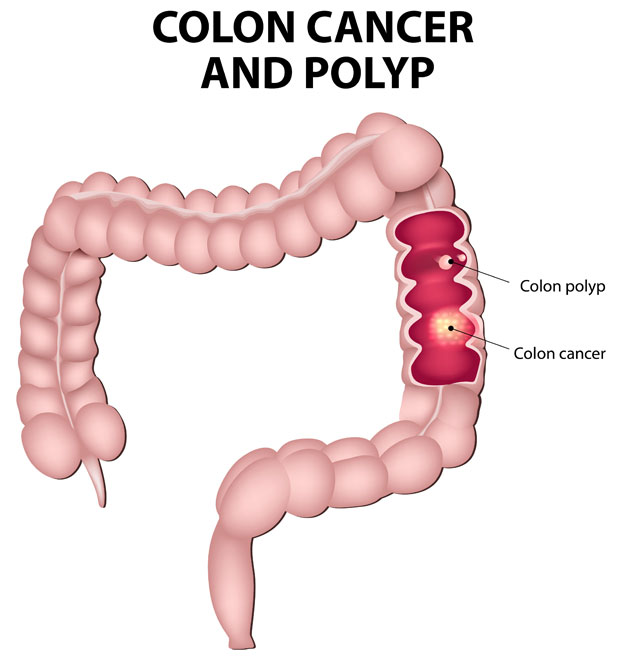
Here is the part that surprises many patients. Colorectal cancer often begins as a small, harmless-looking lump on the inner wall of the bowel, a growth called a polyp. Not every polyp turns dangerous. Some sit there quietly for years. A few, though, slowly change at a cellular level, and that is where trouble starts.
How a Tumour Forms
Inside the lining of your gut, cells are constantly being replaced. It is a tidy, well-managed process most of the time. Occasionally, the instructions go wrong. Faulty cells in the colon or rectum grow when they should rest, and they multiply uncontrollably, building up into a mass rather than dying off as they should.
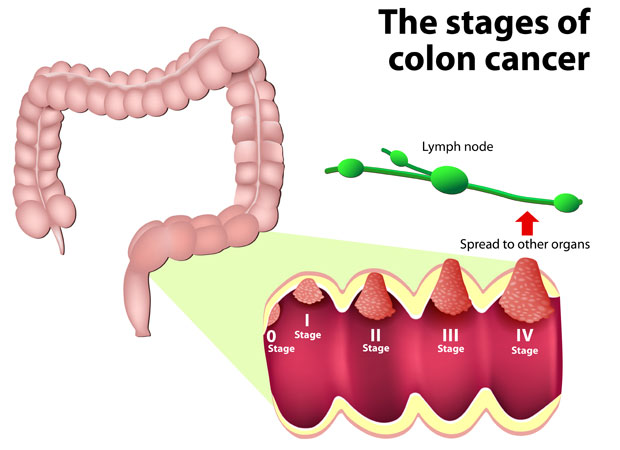
When colon cancer occurs, those abnormal cells can stay contained for a while, which is precisely why early detection matters so much. Left alone, the disease may push deeper into the bowel wall and, eventually, reach nearby lymph nodes or other organs. Found at the polyp stage, the outlook is excellent. Found late, things get harder.
A Quick Word on Terminology
You will see several terms used almost interchangeably, and it helps to know they overlap:
- Bowel cancer, the everyday term you’ll hear from friends and family.
- Colon cancer, when the tumour sits in the lower part of the colon.
- Rectal cancer develops in the final segment near the anus.
All three fall under the colorectal umbrella, and the same broad principles of detection apply to each.
Symptoms and Who Is Most at Risk
This is the section people skim, then re-read. Worth slowing down for.
Plenty of cases produce no symptoms at all in the beginning, which feels unfair but is true. Still, certain signs deserve a phone call to your doctor rather than a wait-and-see approach.
Symptoms Worth Acting On
- A lasting change in your bowel habits, whether that is looser stools, constipation, or a sense that you can’t fully empty.
- Blood in the stool, either bright red or darker and tar-like.
- Cramping or stomach pain that simply won’t settle.
- Losing weight without trying, which understandably alarms people, and rightly so.
- Tiredness that rest doesn’t fix, sometimes tied to a low iron count.
None of these guarantees cancer! Piles, infections, and dietary quirks cause the very same things. But blood and persistent change, in particular, should never be brushed aside, especially past your mid-forties.
Risk Factors You Can and Cannot Change
Some risks are baked in. Others are genuinely within your control, which is oddly reassuring once you think about it.
|
Risk Category |
Examples |
Can You Influence It? |
|
Age |
Most cases appear after 50, though younger adults are increasingly affected |
No |
|
Family history |
A close relative diagnosed, or inherited conditions such as Lynch syndrome |
No |
|
Personal history |
Previous bowel polyps or long-standing inflammatory bowel disease |
Partly, through monitoring |
|
Lifestyle factors |
Red and processed meat, low fibre, smoking, alcohol, inactivity, excess weight |
Yes |
That last row matters. Colorectal cancer is the third most common cancer globally, and a meaningful share of the risk traces back to everyday habits. You cannot rewrite your genes. You can, however, eat more vegetables, move a bit more, and cut back on the cigarettes and the wine.
Screening, Diagnosis and Getting Answers
Screening is the unsung hero of this whole story. It finds disease before symptoms ever appear, and sometimes it stops cancer from forming altogether by catching polyps along the way.
Why Screening Saves Lives
Regular bowel screening is the single most effective tool we have for early detection. The logic is plain: a polyp spotted and removed during a routine check never gets the chance to turn nasty. People often delay because the topic feels embarrassing, or they assume no symptoms means no problem. Both assumptions cost lives. If you are over 50, or younger with a family history, screening should be on your radar.
How Doctors Confirm a Diagnosis
When something needs checking, a surgeon draws on a range of tools to work out exactly what’s going on. The aim is a clear answer, fast, so you are not left guessing.
- Colonoscopy, the gold standard, lets the doctor view the entire colon and take tissue samples in one sitting. Dr Markides is an accredited colonoscopist certified by the Joint Advisory Group (JAG) in the UK and can refer you to the appropriate specilaists.
- Flexible sigmoidoscopy, a shorter look at the lower bowel when that is all that’s required.
- Biopsy, where a tiny sample is examined under the microscope to confirm whether cancer cells are present.
- Imaging such as CT or MRI scans, used to see how far, if at all, the disease has spread.
Once someone is diagnosed, the next conversation is about staging, that is, how advanced the tumour is. Staging shapes everything that follows, from the type of operation to whether extra treatment is needed. It also explains why two people with the same diagnosis can be told quite different things.
How Colorectal Cancer Is Treated
People naturally want to know what happens after a diagnosis, so here is the short version. This page is a starting point only; each treatment has its own dedicated page with far more detail, linked below.
Treatment is never one-size-fits-all. It depends on where the tumour sits, how far it has grown, and your general health. Modern care leans on a team approach, with surgeons, oncologists, radiologists, and specialist nurses all weighing in. Surgery, though, remains the mainstay for most colorectal cancers, and a good deal of progress has made it gentler than it once was.
Surgical Approaches at a Glance
Keyhole methods have changed the picture entirely. Rather than one large wound, laparoscopic and robotic techniques use a few small cuts, which generally means less pain, a quicker recovery, and a shorter hospital stay. Not every case suits this route, but for many patients the contrast is significant.
Below are the main surgical options in which Dr Markides specialises, with laparoscopic completion rates over 95%. Each links to a fuller explanation:
- Laparoscopic colectomy and TME surgery, removing the affected section and, for rectal tumours, the surrounding tissue with great precision.
- Central Mesocolic Excision (CME) for colon cancer, a meticulous approach to clearing the tumour and its margins.
- Total Mesorectal Excision (TME) for rectal cancer, the technique that improved outcomes and lowered recurrence rates.
- TAMIS (Transanal Minimally Invasive Surgery), used for certain rectal tumours, a service Dr Markides developed during his UK career.
Treatments Beyond Surgery
Once all the results are available you will be seen in the clinic and the various management options will be discussed with you depending on the stage of the disease, your general health and your expectations. In most cases, treatment takes the form of surgery to remove the cancer, which gives you the best chances of becoming free of cancer. This is commonly a laparoscopic colectomy or anterior resection to remove the part of the affected colon or rectal cancer, respectively, with its blood supply and lymph glands. In some cases chemotherapy or radiotherapy or a combination of the two may be needed prior to the operation in order to shrink the cancer.
|
Stage at Diagnosis |
Typical Approach |
General Outlook |
|
Early (polyp or contained tumour) |
Removal during colonoscopy or keyhole surgery |
Very favourable |
|
Localised but invasive |
Surgery, sometimes with chemo or radiotherapy |
Good, with timely care |
|
Spread to lymph nodes |
Surgery plus chemotherapy |
Variable, often manageable |
|
Advanced or metastatic |
Combined systemic therapy, selective surgery |
Focus on control and quality of life |
The table simplifies things, naturally. Every patient is different, and the right plan only becomes clear once staging is complete.
Understanding Your Care in Cyprus
Why does the surgeon behind the information matter? Because experience and judgement are not interchangeable, and in cancer work the small details count.
Dr Georgios Markides trained for seventeen years in the United Kingdom, graduating with honours from the University of Manchester before completing higher surgical training in some of the country’s largest teaching hospitals. He holds the Certificate of Completion of Training (CCT) from the General Medical Council, a Master’s degree in Advanced Surgical Practice awarded with Distinction, and recognition from the Association of Coloproctology of Great Britain and Ireland for his colorectal subspecialty. In 2016, he became a permanent Consultant Colorectal Surgeon at the Royal Blackburn Teaching Hospital, managing thousands of emergency and elective cases. Moving his practice to Cyprus in 2018, he has since performed thousands more procedures. He specializes in advanced colorectal cancer surgery, personally undertaking over 100 major colorectal oncological operations per year with an impressive 95%+ laparoscopic success rate.
What patients tend to mention, though, isn’t the list of credentials. It’s the manner. He explains things plainly, never rushes, and treats people as people rather than case numbers. Based at the Apex Building in Strovolos, Nicosia, the clinic serves patients from across Cyprus, including Larnaca, Limassol, Paphos and Famagusta, with in-clinic diagnostics that mean fewer trips and faster answers.
Frequently Asked Questions
Is colorectal cancer curable if caught early?
Yes, and the difference early detection makes is striking. When the disease is found at the polyp stage or while still contained within the bowel wall, surgical removal alone often cures it, with survival rates above 90 percent. This is exactly why screening matters so much. Dr Georgios Markides, a UK-trained colorectal surgeon in Cyprus, can arrange a colonoscopy and, where appropriate, remove suspicious growths during the same procedure, frequently before they ever become dangerous.
What is the difference between colon cancer and rectal cancer?
Both fall under the colorectal heading and start in the large intestine, but their locations set them apart. Colon cancer develops in the lower part of the bowel, whereas rectal cancer forms in the final few centimetres before the anus. That distinction affects treatment: rectal tumours often need radiotherapy and a specialised operation called Total Mesorectal Excision. Understanding which type you have is one of the first things a surgeon will clarify after diagnosis.
At what age should I start bowel screening in Cyprus?
For most people with average risk, screening conversations should begin around age 50. If you have a family history of bowel cancer, inherited syndromes such as Lynch syndrome, or previous polyps, you may need to start earlier and screen more often. Anyone noticing blood in the stool, persistent changes in bowel habits, or unexplained weight loss should seek advice regardless of age.
Does keyhole surgery work for bowel cancer?
For many patients, yes, and it brings real benefits. Laparoscopic and robotic techniques use several small cuts instead of one large incision, which usually means less post-operative pain, a shorter hospital stay, and a faster return to normal life. Not every case suits this method; some tumours require open surgery. Dr Georgios Markides assesses each patient individually and has extensive experience in minimally invasive colorectal procedures built across his UK and Cyprus career.
How is colorectal cancer diagnosed?
Diagnosis usually starts with a colonoscopy, which lets a doctor inspect the full length of the colon and take a tissue sample if anything looks abnormal. That sample, or biopsy, is examined under a microscope to confirm whether cancer cells are present. Scans such as CT or MRI then show whether the disease has spread, a process known as staging. Together, these steps give a clear picture and guide every decision that follows.
Learn More About Bowel Health and Screening
Knowing the signs is the first step, and you don’t have to work it all out alone. If you would like to understand your own risk, or simply talk through symptoms that have been bothering you, clear and honest information is within reach.
Read more about screening and diagnosis, or find out how Dr Georgios Markides supports patients across Cyprus from first consultation onward.
Choose Category
– Colorectal cancer
– Colorectal polyps
– Diverticulosis
– Ulcerative colitis and Crohn’s
– Stoma
– Abdominal pain
– Constipation
Need to contact us or book an appointment?
Disclaimer
The information relating to general and colorectal disorders and their treatments given on this website is not complete and is not intended as a substitute for a consultation with your doctor. Always seek medical advice from your doctor before making a decision about any of the conditions and/or treatments mentioned on this website.
© Dr Georgios Markides
Contact Information
You can always contact our Clinic for booking appointments and other useful information:
Dr. Georgios Markides,
Consultant General & Colorectal Surgeon
APEX Building, 47 Andreas Avraamides Str., 2024 Strovolos, Nicosia, Cyprus